
PARAGON-HF: Sacubitril-valsartan in heart failure with ejection fraction >=45%
By Hans Haag with editorial support from Ricky Turgeon
PARAGON-HF. NEJM 2019;381:1609-20
Bottom line:
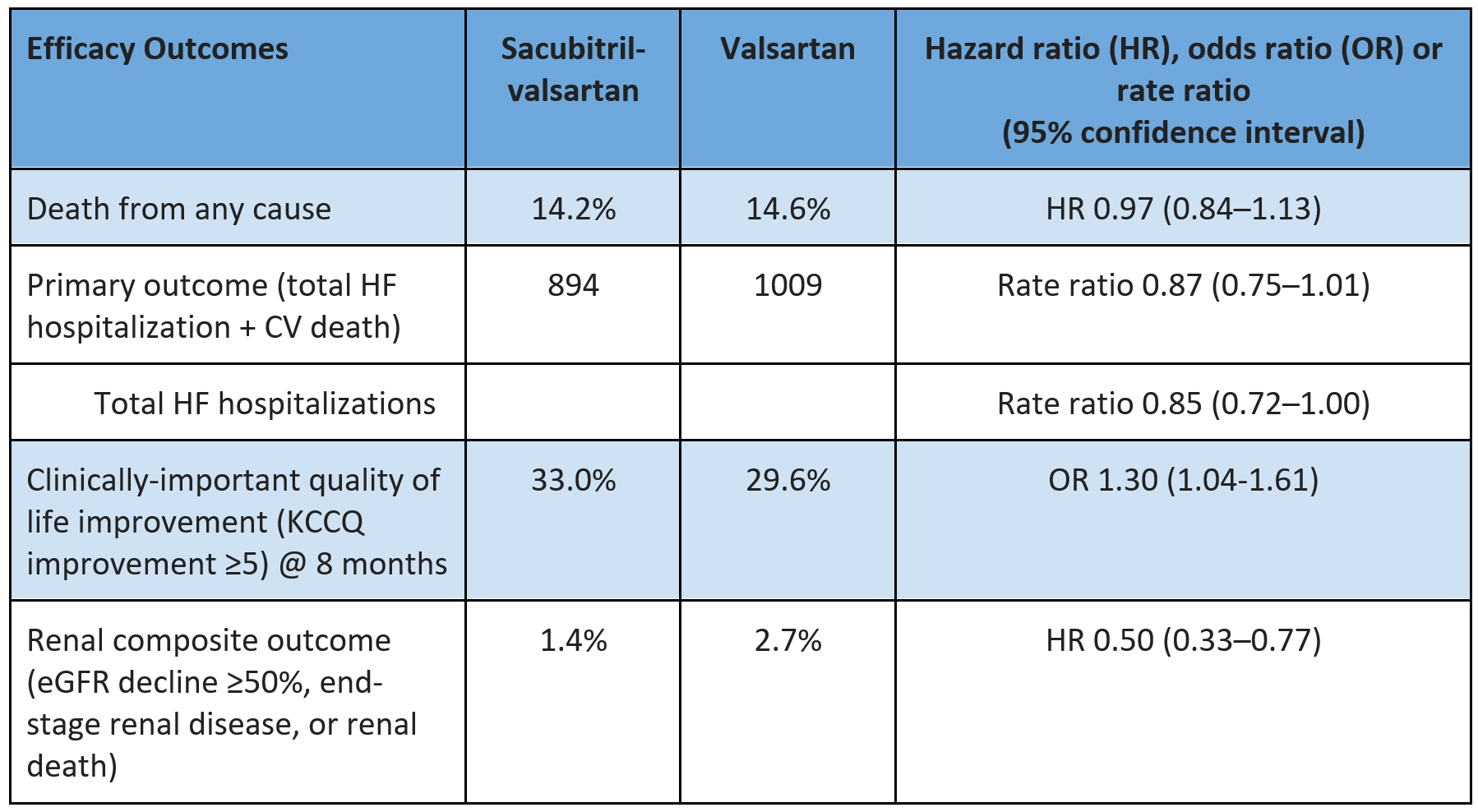
In patients with heart failure (HF) with left ventricular ejection fraction (LVEF) ≥45%, sacubitril-valsartan did not reduce the composite total HF hospitalizations/cardiovascular (CV) death or death from any cause over ~3 years.
Sacubitril-valsartan increased the risk of hypotension (+5%) and angioedema (+0.4%) compared with valsartan.
In subgroup analyses (which often lead us astray) sacubitril-valsartan reduced HF hospitalizations in females by ~1.5%/year (but not males) with LVEF in the “lower” range (45-60%).
Patients (n=4822 randomized)
Screened 10,359 -> 5746 entered valsartan run-in (~9% discontinued) -> 5205 entered sacubitril-valsartan run-in (7% discontinued) -> 4822 randomized
Included:
Age 50+
NYHA 2-4
LVEF ≥45% measured in the last 6 months
At least one of the following:
HF hospitalization within 9 months prior + NT-proBNP >200 pg/mL (>600 pg/mL if AF)
NT-pro-BNP >300 pg/mL (>900 pg/mL if AF)
Echo evidence of LA enlargement (e.g. LAV ≥55 mL or LAVi ≥29 mL/m^2) or LVH (septal thickness ≥1.1 cm)
Symptomatic HF for at least 30 days prior to screening visit
Structural heart disease (LA enlargement or LVH)
Key exclusions:
Any prior LVEF <40%, history of dilated cardiomyopathy, hemodynamically significant valvular heart disease
Uncontrolled/life-threatening dysrhythmia, including AF-RVR
History of angioedema
Alternate diagnosis to explain HF symptoms (e.g. anemia with Hb <100 g/L, severe COPD)
Uncontrolled hypertension
SBP <100 mm Hg or symptomatic hypotension
eGFR <30 mL/min/1.73m^2 or a reduction of >35% after run-in period
K >5.2 mmol/L
Baseline:
Age 73, 52% female, 82% white, 12% Asian, 2% Black
NYHA 2 (77%) & 3 (20%), LVEF median 57%, NT-proBNP ~900 pg/mL, HF hospitalization in last 12 months ~23%
Comorbidities: HTN 96%, diabetes 43%, AF/AFlutter 33%
Meds: Diuretic 96%, ACEI/ARB 86%, beta-blocker 80%, MRA ~25%
SBP 130, eGFR 63
Interventions: Sacubitril-valsartan 97/103 mg BID vs valsartan 160 mg BID
Intervention: Sacubitril-valsartan 97/103 mg BID (82% on target dose)
Comparator: Valsartan 160 mg BID (85% on target dose)
Co-intervention: MRA permitted, all other non-study RAAS inhibitors stopped
Outcomes @ median 35 months (2.9 years)


Internal validity: Low risk of bias selection, performance, detection & attrition bias
Selection bias: Computer-generated random sequence; allocation concealment by interactive web-response system
Performance & detection bias: Patients, clinicians & investigators blinded to study allocation via double-dummy placebo
Attrition bias: ITT analysis, LTFU <0.1%
Other considerations
Generalizability:
16% excluded in single-blind run-in
Consisted of (1) Valsartan 40-80 mg BID x 1-2 weeks, then (2) sacubitril-valsartan 49/51 mg BID x2-4 weeks, then randomized
PARAGON-HF defined “preserved” ejection fraction as >45%, which differs from the (subsequent) 2021 universal definition and classification of HF’s classification of HF with preserved LVEF as ≥50% and HF with LVEF 41-49% as mildly-reduced
Pre-specified subgroup analysis of the primary outcome based on baseline LVEF suggests greater benefit with ARNI in patients with LVEF below the study median (≤ 57%) and in females (but no reduction in death in any subgroup)
In females, (for the outcome of first HF hospitalization) this translates to a reduction from 7.2%/y with valsartan down to 5.5%/y with sacubitril-valsartan (-1.7%/y)
A secondary paper further elicited an interaction between sex*LVEF and ARNI response:
Consistently no benefit for the primary outcome in males, regardless of LVEF
Benefit in females with LVEF ≤60%, with greater relative efficacy as LVEF decreased
This interaction has also been seen with candesartan (ARB) and spironolactone (MRA)

Are the results clinically important?
Yes for: Patients who place higher value on reducing HF hospitalizations and improving quality of life than they do the increase in hypotension, angioedema (and higher cost)
Not for:
Males
Female patients with LVEF ≥60%
Female patients who do not care about the benefits noted above, or who are more concerned about costs, pill burden, and the adverse effects noted
However, given the more robust evidence and greater certainty for SGLT2 inhibitors and MRAs in this setting (noted below), ARNI should generally be offered after exhausting those other options.
Context
Pharmacotherapeutic options for HF with LVEF >40% (including HF with mildly-reduced [41-49%] and preserved [≥50%] LVEF) are limited, with strongest evidence for MRAs and SGLT2i (published after PARAGON-HF); these medications reduce HF hospitalizations, but not death.
Sacubitril targets the natriuretic peptide pathway by inhibiting neprilysin
Neprilysin is an enzyme that degrades natriuretic peptide (as well as “off-target” hormones, most importantly bradykinin)
Natriuretic peptides directly induce natriuresis, diuresis, peripheral vasodilation, and inhibit cardiac remodeling, and suppress the renin-angiotensin system.




